



La parodontopatia (infiammazione dei tessuti gengivali,sanguinamento) e la recessione del supporto osseo delle arcate dentarie, costituisce il primo passo che porta alla Malattia Parodontale, nota come “Piorrea”. La manifestazione di questi segni impone una valutazione clinica approfondita ed integrata con esami strumentali che consentano di indagare anche gli aspetti funzionali del sistema masticatorio.

Lo Studio Calzavara è una struttura odontoiatrica polifunzionale sviluppata al massimo livello tecnologico e strumentale. L’utilizzo del microscopio operatorio, consentendoci interventi microinvasivi, ci permette di migliorare i risultati terapeutici in tutti i campi dell’odontoiatria.
Il termine “Malattia parodontale” indica le patologie del parodonto. La causa principale di questo insieme di malattie sono i batteri, che colonizzano le superfici dei denti sotto forma di placca e tartaro. Con un’azione lenta, i batteri inducono una progressiva perdita del tessuto di supporto dei denti, con formazione di una “tasca parodontale”

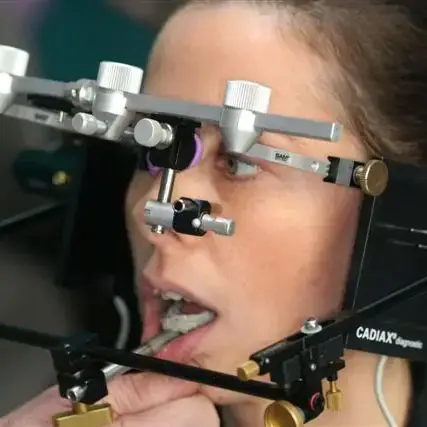
L’apparato masticatorio costituisce un sistema complesso dove i tanti piani funzionali presentano un rapporto angolare armonico tra di loro; questo apparato si inserisce in un sistema organico ancor più vasto col quale interagisce. Pertanto l’odontoiatria non può continuare ad essere confinata allo studio dell’ingranaggio dei denti ma deve studiare le complesse relazioni tra apparati integrati.